Middle Lobe Atelectasis
Pathophysiology: Simplest approach is extramural, intramural and
luminal mechanisms impacting the bronchus.
Extramural: contiguous tumors/masses, fibrosis with
traction atelectasis
Intramural: cancer; endobronchial metastasis; carcinoid,
benign tumor or polyp; bronchostenosis with or without
bronchiectasis (TB)
Luminal: mucus plug, foreign body, aspirant, blood, or
pus
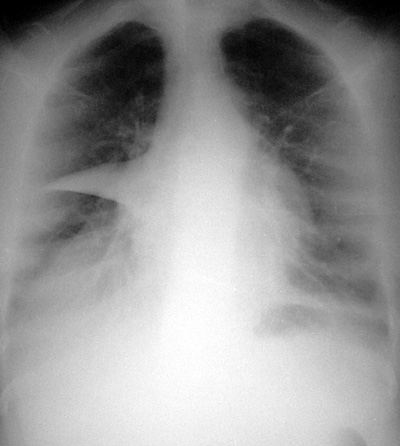
CXR Findings: Classic silhouette sign with loss of the
right heart border (RML) or left heart border (lingula). The
lateral film may show displacement of the minor fissure and
right oblique fissure with ōpie shapedö density on lateral film
in RML collapse.
Clues: The volume of the middle lobe and lingula is too
small to generate shifts of the hemidiaphragms or mediastinum,
so donÆt expect to see these.
Technique Tip: Lordotic views show RML and lingular
atelectasis well.
Clinical Clue: Often existing or predisposing pneumonia,
bronchiectasis, and a central cancer. Follow patient and CXR to
resolution. May need CT and bronchoscopy to exclude central
cancer.
ōAunt Sophiesö:
- Right middle lobe pneumonia: often associated with some degree of volume loss
- Right middle lobe bronchiectasis: eg. “middle lobe syndrome” in TB, atypical TB
- Post-obstructive pneumonias: need to rule out central cancer or tumor which is blocking right middle lobe bronchus. May need CT and/or bronchoscopy.
|