Mitral Stenosis
Pathophysiology: The commonest etiology is rheumatic heart
disease. A spectrum of worsening physiologic changes occurs
paralleling the severity and duration of the mitral stenosis.
These go along with increasing wedge pressure measurements.
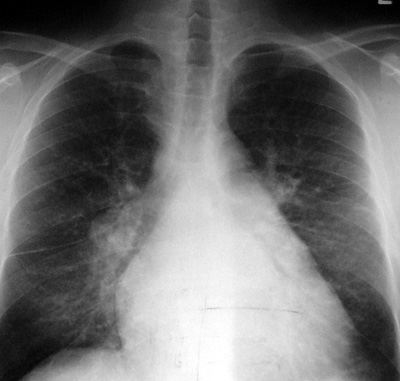
These changes are reflected in the plain CXR as:
1.
left atrial hypertrophy then dilatation
2.
prominence of the left atrial appendage (if present)
3.
pulmonary venous hypertension and vascular redistribution
4.
right ventricular hypertrophy then dilatation
5.
central perihilar interstitial pulmonary edema
6.
airspace pulmonary edema
CXR Findings:
1.
enlarged left atrium
2.
enlarged left atrial appendage
3.
straightening of the left heart border (“mitralization”)
4.
vascular redistribution
5.
right ventricular dilation
6.
interstitial pulmonary edema in perihilar region with:
−
perivascular fuzziness
−
peribronchial cuffing
−
Kerley B lines
−
Kerley A lines
7.
airspace pulmonary edema
8.
mitral valve calcifications
9.
pleural effusions associated with CHF
Clues:
Normal wedge pressure: 5 mm Hg
Vascular redistribution: wedge pressure 18 mm Hg
Interstitial pulmonary edema: wedge pressure 22 mm Hg
Airspace pulmonary edema: wedge pressure >25 mm Hg
“Aunt Sophies”: Very few in typical or classic cases.
May consider cardiomyopathies, CHF (other causes), and
left-to-right shunts.
|