|
 |
SCOUT
AP VIEW
Shows a calculus within the Kockĺs pouch |
SCOUT
LATERAL VIEW |
 |
 |
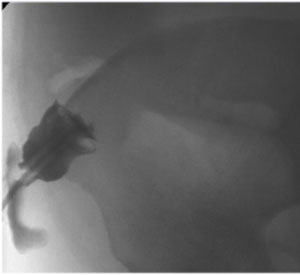
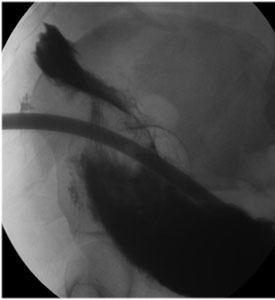
POUCHOGRAM LATERAL OBLIQUE VIEW
A catheter has been inserted into the lumen of the valve and
contrast shows the outline of the cutaneous portion of the
valve. |
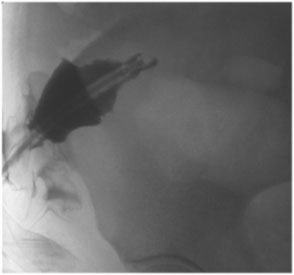
POUCHOGRAM LATERAL OBLIQUE VIEW
The catheter has been advanced further in to outline more of the
valve. |
 |
 |
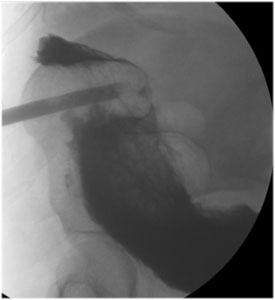
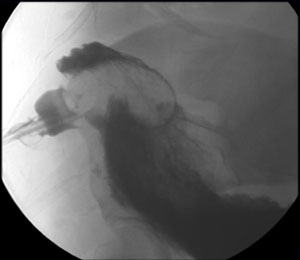
POUCHOGRAM LATERAL OBLIQUE VIEW
The catheter has been advanced further into the pouch. More
contrast is instilled which outlines the valve to better
advantage. Notice there is some contrast outlining the superior
portion of the valve. This is suggestive of a Ĺslipped valveĺ. |
POUCHOGRAM LATERAL OBLIQUE VIEW |
 |
 |
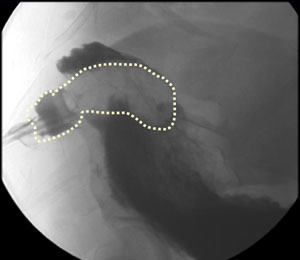
POUCHOGRAM LATERAL OBLIQUE VIEW
Withdraw the catheter and drip contrast again to show the entire
Kockĺs valve (dotted line). |
POUCHOGRAM LATERAL OBLIQUE VIEW
Then withdraw the catheter and drip contrast again to show the
entire Kockĺs valve |