This procedure is done on patients who
have had a total colectomy with an Ileo-Anal Reservoir anastomosed
at the anal verge. This procedure is done mostly for patients with
ulcerative colitis, colonic polyposis and sometimes for colonic
cancers.
The pouchogram is done to assess for leaks or other long term
complications such as strictures at the ileo-anal anastomosis or the
pouch itself; sometimes to assess the capacity of the pouch.
Most leaks occur in the immediate post-operative period and are
located at the ileo-anal anastomosis especially the posterior
aspect; therefore during fluoroscopy the patient should be first n a
lateral position to assess the pouch. Then one can fluoroscope in an
oblique and AP position to check for leaks at the lateral aspect of
the anastomosis.
Equipment
- 12F Foley catheter
- Xylocaine gel
- Toomey Syringe
- Clamp
- Contrast:
- Hypaque 30% (unless otherwise stated)
Technique
The study can be performed through an existing rectal tube or one
can inset a small (12 F) Foley catheter into the pouch.
DO NOT INFLATE THE BALLOON. The
Foley catheter balloon is not inflated so that leaks at the ileo-anal
anastomosis are not obscured. Sometimes the surgeon may ask to check
the pouch via the DISTAL LOOP ILEOSTOMY opening. It is best
to confirm the route of the examination with the surgeon.
The contrast used is almost always HYPAQUE 30% concentration.
Radiographs
Scout film, lateral, L.A.O., R.A.O. and AP views with
contrast.
In patients who have been operated on more than 4 weeks, one should
do a STRAINING view in AP and lateral
projections. Please split films to minimize film usage.
A POST-EVACUATION view is also done in some patients who are
being assessed for pouch integrity and ileostomy closure. Both AP
and lateral views are done on a single 8x10 radiograph split.
Barium (30% w/v) may be used for patients being assessed for
long-term complications.
 |
 |
LATERAL
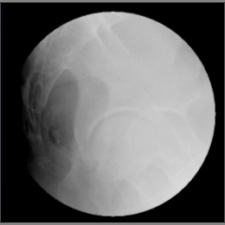
SCOUT VIEW:
Both AP and lateral scout radiographs are done. These views will
assess the amount of air in or behind the pouch or in the vagina
(in case of an ano-vaginal fistula). This view will localize the
bowel sutures which can mimic a leak after contrast has been
instilled into the pouch.
All images are taken on 9" FOV.
|
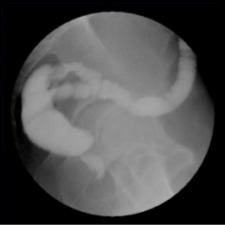
POUCHOGRAM:
The pouch is filled with small quantities of contrast and
checked fluoroscopically for any leaks. Images are taken mostly
in the lateral position where leaks are best detected (either
posterior or anterior at the ano-pouch junction – arrow). |
 |
 |
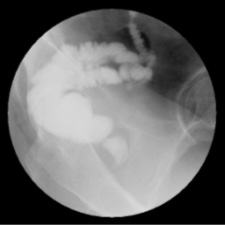
OBLIQUE
VIEW:
This view ensures that there are no subtle postero-lateral
leaks. The anal canal must be opacified on ALL views to
ensure proper and complete evaluation of the ileo-anal
anastomosis. |
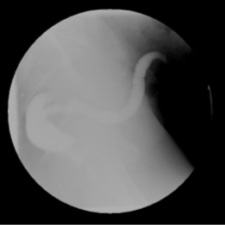
AP
VIEW:
This will ensure detection of possible antero-lateral leaks.
If the anal canal cannot be opacified on any views, ask the
patient to perform a Valsalva maneuver. This will serve
two purposes: to fill the anal canal and to show any small
leaks.
|
 |
 |
AP.
VIEW:
Taken with 12” FOV to show the entire pouch and the ileostomy
opening. |
LATERAL
VIEW:
Taken with 12” FOV to show the entire pouch and the
ileostomy opening.
|
 |
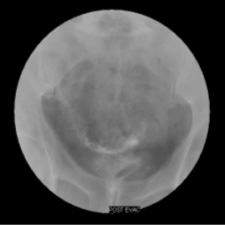 |
POST
EVACUATION VIEW:
The catheter is removed and the patient is asked to evacuate the
pouch contents. This is to assess the post evacuation residue
and sometimes a leak occurs after the forced evacuation of the
contrast. |
POST
EVACUATION VIEW:
Both AP and Lateral views are taken. Most leaks occur at
the posterior aspect of ileo-anal pouch anastomosis. Other sites
include anterior, lateral anastomosis and at the blind ended
‘afferent limb’. Rarely, the leak can occur at the midline
suture line of the pouch. There may also be an ano-vaginal
fistula |
|