 |
 |
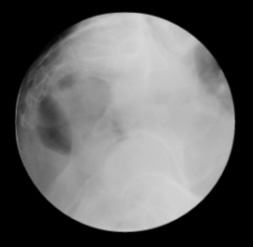
SCOUT LATERAL VIEW:
This will assess if there is any air in the vagina. Do
NOT inflate the balloon as this
will obscure the fistula. |
SCOUT AP VIEW:
Dilute barium (30-05 % w/v dilution of Polibar 100%) or 30-60%
Hypaque contrast can be used. |
 |
 |
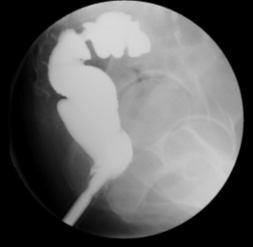
LATERAL VIEW:
This is the most important view. The early filling phase
should be done carefully and using fluoroscopy to detect the
ano-vaginal fistula early. |
OBLIQUE VIEW:
This view will help detect some of the unusual leaks along the
lateral aspect of the ano-rectal junction. |
 |
 |
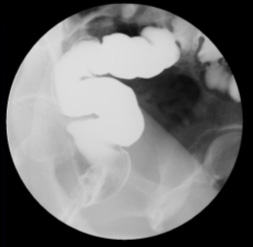
AP VIEW:
Sometimes introducing air can show the fistula better. |
SPECIAL MANUVERS:
Withdraw the rectal tube down to anus & have patient perform
the Valsalva maneuver. |
 |
 |
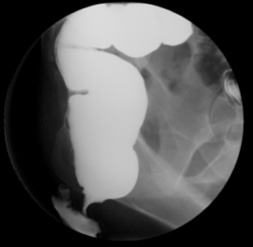
SPECIAL MANEUVERS
(LATERAL VIEW):
Remove the rectal tube and ask the patient to perform the
Valsalva maneuver. |
SPECIAL MANEUVERS
(AP VIEW):
Remove the rectal tube and ask the patient to perform the
Valsalva maneuver. |