|
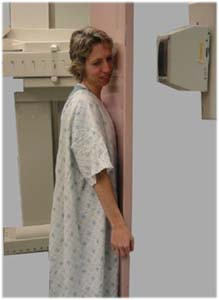
Single Contrast Esophagram Views: |
|
 |
 |
| The
patient is positioned Upright and in the Left Posterior Oblique
(LPO) position for the esophagogram. The patient is asked
to drink a small volume of high density barium (e.g. EZHD) and a
single contrast view is done. This initial view is done to
ensure there is no large obstructing lesion present prior to
giving the effervescent granules. |
Single
contrast:
A small bolus of barium is given. |
|
Effervescent Granules: |
|
 |
 |
|
The patient is then given 1 packet of gas granules followed by
ONLY 15 cc of water. |
|
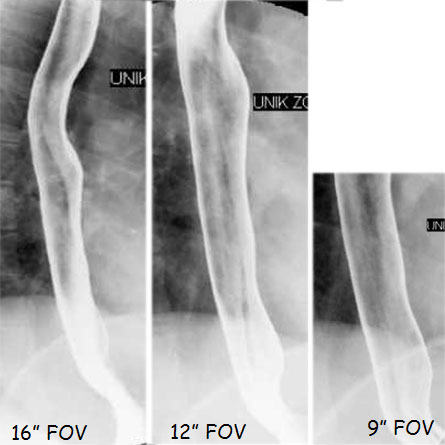
Double Contrast Esophagram Views: |
|
|
The patient is asked to drink the rest of the barium
continuously. Views of the entire esophagus in double contrast
are taken from the cervico-thoracic junction to the esophago-gastric
junction. The esophago-gastric junction area is imaged at 9” FOV
to assess fine detail. The double contrast views are necessary
especially for reflux disease (i.e. detecting early signs of
esophagitis, etc). |
|
 |
|
Coating the Stomach: |
|
|
 |
The patient is placed in the PRONE (facing the table) position
and the table is brought down. This will allow for better
coating of the anterior wall of the stomach. To coat the rest of
the stomach, the patient does the ‘log roll’ (i.e. the patient
is turned from prone onto the left lateral decubitus position,
followed by supine, right lateral, prone then left lateral
decubitus and finally supine position). This maneuver will keep
all the barium in the fundus. |
|
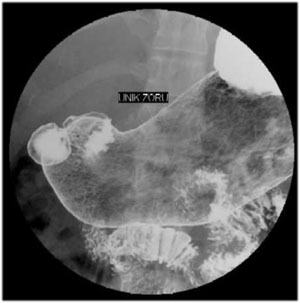
Left Posterior Oblique View of the Gastric Antrum: |
 |
 . . |
|
The patient is then placed in a Left Posterior Oblique (LPO)
position. This view allows you to visualize the gastric antrum
and the duodenal cap while being able to sweep in double
contrast phase. |
Double contrast image of the gastric antrum taken on 9" FOV. |
|
Right Posterior Oblique Views of the Lesser & Greater
Curvatures: |
 |
This view is taken to assess the lesser and
greater curvatures of the body of the stomach. This view splits
the barium into two portions – one in the fundus and the second
in the antrum. This view allows the maximum evaluation of the
two curvatures in double contrast. |
|
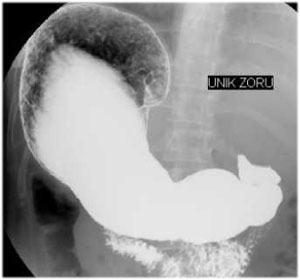
Right Lateral Decubitus Views of the Gastric Fundus
(Double Contrast): |
|
With the patient in the Right Lateral Decubitus
position, a view of the gastric fundus in double contrast is
taken first on 16” FOV followed by 12” FOV. This traps the air
and gives one of the better images of the fundus (before patient
has the urge to burp). |
 |
 |
|
Right Semi-Prone Oblique Views of the Doudenal Cap (Single
Contrast): |
|
One must take at least two or three views of the
duodenal cap in different projections and angulations. |
|
|
|
|
Prone View of the Entire Stomach & Duodenum: |
 |
This view is like the ‘compression’ of the
antrum in single contrast. The fundus is in double contrast and
the duodenal sweep is sometimes seen to a better advantage. |
|
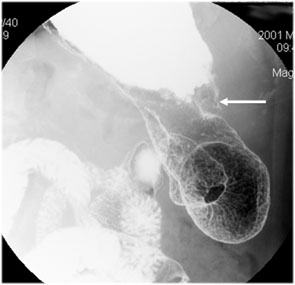
Left Lateral Decubitus View of the Anterior Stomach Wall: |
 |
 |
|
The patient is then turned to the Left lateral
Decubitus position. This view will provide a double contrast
view of the anterior wall of the stomach and sometimes of the
posterior portion of the fundus. |
NOTE: There is a lesion on the anterior wall of
the stomach (arrow) |
|
Supine View of the Entire Stomach & Duodenum: |
|
 |
 |
|
With the patient in Supine position, a final view of the gastric
body and antrum (in double contrast) and the duodenal sweep
(single contrast) is taken. |
The final image is taken of the entire stomach including views
of barium filled duodenal sweep up to the ligament of Treitz |
|
Drinking Esophageal Peristalsis View: |
 |
|
|
This view is taken with the patient in a
semi-prone position with the left arm by the side and right hand
used for holding the drinking cup. The patient drinks Polibar
100% quickly and a cine esophagogram from the cervical to the
esophago-gastric junction is taken (using ‘last image hold at 2
frames fluoroscopic image) and 16” FOV. One may do this view
early if there is pyloric spasm. |
|
Upright Gastric & Duodenal Views: |
|
|
This view is taken to assess the distensibility
of the antrum (in single contrast with the weight of barium) and
double contrast views of the fundus. For the fundus, oblique &
lateral views may be helpful. |
|
|