Pneumocystis Carinii Pneumonia (PCP)
Pathophysiology: Pneumocystis carinii is a
ubiquitous organism. It is not pathologic in the normal host
but is pathologic in immunocompromised hosts especially those
with HIV. It is not a community acquired pneumonia (CAP) and is
not spread from host to host. An inflammatory process begins in
interalveolar walls with desquamation of alveolar cells leading
to diffuse alveolar damage and varying degrees of inflammatory
reaction.
Clues:
1. The
CXR presentation has changed over the years. At the beginning of
the HIV epidemic, PCP patients often presented in acute
respiratory failure with an ARDS lung pattern.
2.
PCP often presents with co-existing pneumonias and
superinfections.
3.
Commonest pneumonia in HIV patients is still CAP.
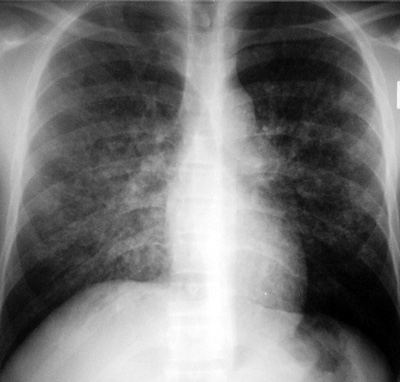
CXR Findings:
1.
Classic: peri and infra hilar interstitial changes
which coalesce
2.
Infrahilar inverted triangle-like densities from the hila
to the lung bases
3.
Many variations: diffuse airspace changes, rarely nodular
areas, rarely cavitary areas
4.
Pleural reactions NOT marked; small effusions may be seen
5.
NOT associated with significant adenopathy on plain films
6.
Definite association with pneumothoraces
Complications/Associations in HIV patients:
1.
Non T-cell Lymphoma
2.
Kaposi's sarcoma with lung metastases
3.
Tuberculosis and atypical tuberculosis especially MAI
4.
Pneumothoraces
“Aunt Sophies”: (with appropriate history, easy to diagnose
in its typical form)
1.
Pulmonary edema or ARDS pattern
2.
CAP
3.
Tuberculosis (typical and atypical)
|