|
|
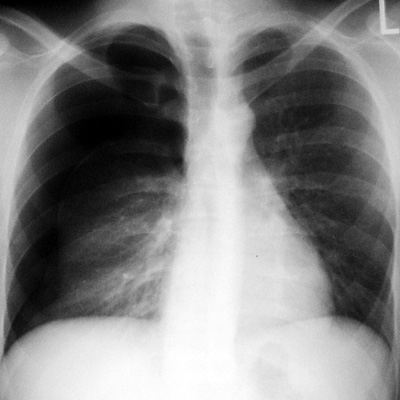
Pneumothorax
Pathophysiology: Any process allowing atmospheric air to
enter the potential pleural space leads to reduction of negative
intrapleural pressure and varying degrees of lung collapse. The
dreaded complication is a tension pneumothorax. In this
case, the air enters the pleural space and a flap valve-like
effect occurs with less air leaving the pleural space on
expiration than entering on inspiration. As a result, the
pleural space progressively inflates, deviating the mediastinum,
increasing lung compliance and compressing the great veins.
Commonest causes:
-
Spontaneous:
typically in young tall athletic patients, often recurrent
-
Associated with
many interstitial lung diseases and infections (eg. PCP,
interstitial fibrosis)
-
Trauma: fractured
ribs; stab and bullet wounds
-
Iatrogenic
following needle biopsy, central line insertion or
thoracentesis
-
Rupture of
peripheral blebs and bullae especially in patients with
bullous emphysema
-
Infections, usually
granulomatous lung disease (eg. tuberculosis)
-
Rarely, with tumor
destruction of airways
CXR Findings:
-
Classic sign: Visceral
pleural sign: the line of the visceral pleura is seen
outlining the collapsed lung
-
No airways or
vessels beyond visceral pleura of collapsed lung
-
May be dynamic
movement of mediastinum on inspiration and expiration (usually
not useful except if one does fluoroscopy)
-
Tension
pneumothorax: mediastinum shifted contralaterally
-
Superior Sulcus
sign: typical features of pneumothorax seen in upright
patient. In the supine patient, air rises to
anterior and inferior position, giving a circular area of
lucency in the costophrenic sulcus area.
Clues:
-
Tension
pneumothorax is a medical emergency and needs rapid treatment
-
Bright light all
plain films to look for subtle visceral pleural lines
especially in the lung apices
-
Communicate
findings to the referring MD
ōAunt Sophiesö:
-
Tissue folds
-
Rib surfaces may
mimic visceral pleural sign
-
Blebs, bullae and
cavities
-
Severe
emphysematous lung disease
-
Technical factors
with hyperlucency in a lung (eg. rotation)
|
