Rheumatoid Lung Disease
Pathophysiology: An immunologic inflammatory process
involving alveolar walls, small vessels, and mesothelial or
serosal linings (eg. synovium, pleural and pericardial
linings). The inflammatory response leads to granulomata,
diffuse alveolar damage (DAD), vasculitis, fibrosis, exudative
pleural and pericardial effusions, and lung fibrosis.
Clinical Clues: Rheumatoid arthritis is more common in
females, but rheumatoid lung disease is more common in males.
The
pleural effusions are exudative with characteristically very LOW
glucose content (TB effusion has low, but not as low a glucose
concentration)
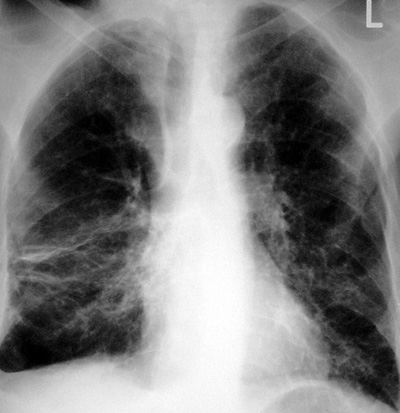
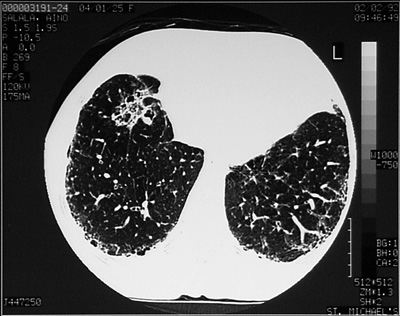
CXR/CT Findings: There are many potential thoracic
manifestations. Listed in order of commonality:
-
pleural effusions
-
diffuse
interstitial lung disease; reticular, with a lower lung
predominance
-
progressive
interstitial lower lung fibrosis and volume loss
-
end-stage lung
disease with honeycombing in the lower peripheral lungs
-
pulmonary nodules
including necrobiotic nodules
-
vasculitis, nodules
and rarely, areas of hemorrhage
-
pericardial
effusion
-
pulmonary arterial
hypertension
-
cor pulmonale
-
Caplan’s
syndrome: synergy between silicosis and rheumatoid lung
disease with larger nodules
“Aunt Sophies”: Many, usually consider a gamut of lower
lung interstitial disease with volume loss.
1.
scleroderma
2.
dermatomyositis (rare)
3.
mixed collagen vascular disease (CREST syndrome)
4.
Idiopathic interstitial fibroisis (UIP, fibrosing alveolitis, cryptogenic fibrosing alveolitis)
5.
Chronic aspiration and lung fibrosis
6.
Drug reactions: rare to have basilar predilection.
|