|

|
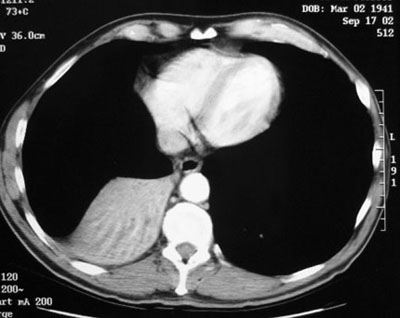
Right Lower Lobe Atelectasis
Pathophysiology: The following mechanisms may lead to lower lobe volume loss or atelectasis:
- Bronchial obstruction or narrowing: any cause: eg. tumor, foreign body, mucus, aspiration, stenosis, extrinsic compression, iatrogenic eg. endotracheal tube misplacement
- Passive or post fibrotic causes: associated with effusions, pneumothorax, marked fibrotic conditions eg. old TB, bronchiectasis
- Post operative: following surgery, especially bypass or thoracic surgery; likely due to mechanical factors and surfactant changes
CXR Findings:
- Classic “sail sign” projecting from right infrahilar area to the hemidiaphragm .
- The normal “greyness” of the heart shadow replaced by “whiteness” of the collapsed RLL
- Loss or silhouetting out of the right hemidiaphragm
- May be mediastinal shift to right
- May be elevation of right hemidiaphragm
Clinical and Radiologic Clues:
- The etiology of the volume loss is often indeterminate on plain films; CT and bronchoscopy are often needed.
- The timing of the atelectasis has diagnostic importance. Acute: aspiration, foreign body, mucus plugging, bleeding and clots. Chronic: tumor, fibrosis, bronchiectasis etc…
- Uncomplicated volume loss is not associated with a pleural reaction
- If there is pleural effusion, need to sort out the relationship: eg. infection, effusion and volume loss, or volume loss due to tumor and malignant effusion etc…
“Aunt Sophies”: There are many. Any moderate to large right effusion will have an element of volume loss.
- Underlying pneumonia and effusion*
- Underlying effusion predominately with secondary or passive atelectasis*
- Pulmonary infarct**
- Any geographic right lower lobe inflammatory or infectious process may be associated with element of volume loss
|
