|

|
Right Upper Lobe Atelectasis
Pathophysiology: Much the same as any other lobe. See “Right Lower Lobe Atelectasis”.
Commonest causes:
- Cancer or tumor involving upper lobe bronchus often at origin of right main stem bronchus. Includes metastases and endobronchial mets
- Post-inflammatory fibrotic diseases permanently tracting the right upper lobe. Includes granulomatous diseases such as TB, fungal diseases, bronchiectasis of any cause (eg. infection, cystic fibrosis), radiation fibrosis, end stage sarcoidosis.
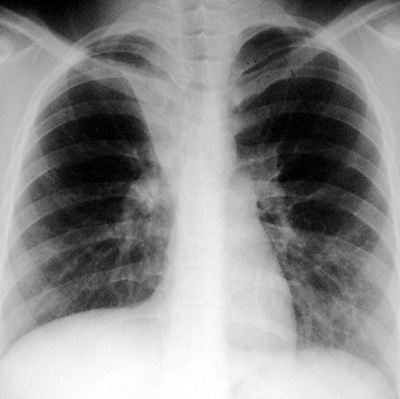
CXR Findings:
Frontal Film:
- typical arcuate elevation of the minor fissure to complete merging of it in upper paratracheal area
- elevation of right hilum
- elevation of right hemidiaphragm
- possible underlying pathology eg. mass or tumor, bronchiectasis etc…
Lateral Film:
- typical convex retrosternal white line of collapsed right upper lobe (not typically seen with left upper lobe atelectasis).
Clinical and Radiologic Clues: (see “Right Lower Lobe Atelectasis”)
- Consider underlying cancer first and exclude
- Consider TB, bronchiectasis, and granulomatous infections
- Think of cystic fibrosis in the right setting
“Aunt Sophies”: Many.
- Almost any airspace process in the upper lobe can be associated with or may mask as atelectasis eg. pneumonia, active TB, etc…
- If trauma history, rule out lung contusion or injury to right upper lobe bronchus
- If asthmatic: mucus plugging
- Bronchiectasis: may be dominant process but fibrosis and traction etc… may lead to some volume loss
- PMF in complicated silicosis
|
