Shunt Vascularity
Pathophysiology: Shunting of the flow of blood from the
systemic side (high pressure) to the venous or pulmonary artery
circulations (low pressure). Usually divided into intracardiac
and extracardiac causes.
Intracardiac Causes:
1.
Atrial septal defects (secundum, primum, high ie. sinus
venosum abnormalities)
2.
Ventricular septal defects: membranous and muscular
3.
Endocardial cushion defects
4.
Coronary artery to vein fistulae (rare)
5.
Admixture anomalies of great vessels (eg. overriding
aorta)
Extracardiac Causes:
1.
Patent ductus arteriosus
2.
Distal arterio-venous shunt: (eg. Paget’s disease,
iatrogenic for hemodialysis)
Clinical Clues: often initially missed clinically and
suspected from CXR
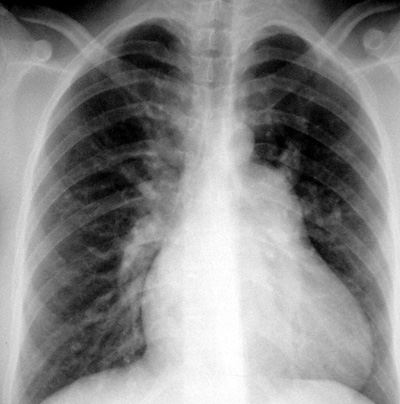
CXR Findings: essentially too much blood flowing through the
lungs at any one time
1.
Prominent central and peripheral pulmonary vasculature
(arteries and veins)
2.
Vessels can be traced further out to the lung periphery
3.
May be associated cardiac abnormalities (eg. enlarged
left atrium, enlarged right atrium)
“Aunt Sophies”: any condition causing increased pulmonary
blood flow (pulmonary pleonemia)
1.
physiologic: exercise, pregnancy
2.
fever, hyperthyroidism, hypermetabolic syndromes
3.
hyperhydration, fluid overload
4.
polycythemia
5.
congestive heart failure
6.
congestive cardiomyopathies
7.
renal failure with fluid overload
Imaging Hint: Do NOT mistake vascular redistribution
for shunt vascularity.
|