|

|
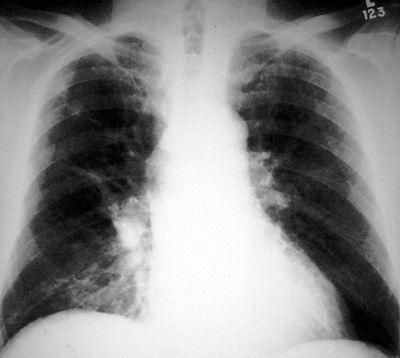
Silicosis
Pathophysiology: An occupational lung disease due to the
inhalation of silica (silicon dioxide crystals). The silicon
dioxide crystals lead to a non-immunologic granulomatous
inflammatory reaction with resulting destruction of alveolar
walls and the lung interstitium. The inflammatory response is
characterized by granulomata, nodules, fibrosis, and reactive
hilar and mediastinal adenopathy.
An
unusual variant: acute silicoproteinosis occurs with
massive exposure to silica in sandblasters. The alveoli fill
rapidly with desquamated epithelial cells and a surfactant-like
substance. The process simulates other air space diseases and
alveolar proteinosis.
Clinical Clues: always an occupational history of mining or
silica exposure.
Almost always in males (social reasons).
CXR/CT Findings:
Simple Silicosis:
-
distinct upper 2/3
lung predilection (due to mechanics of air flow and lymphatic
drainage)
-
small to medium
sized nodules and linear interstitial lung changes
-
characteristic
central hilar and mediastinal adenopathy, often with
egg-shell calcifications
-
may progress to
marked fibrosis, hilar retraction and lung distortion
Complicated Silicosis (see progressive massive fibrosis):
-
PMF
-
Tuberculosis (due
to social conditions of mining and ease of spread)
-
Scar carcinoma (adenocarcinoma
of lung), rarely
“Aunt Sophies”: DDx of upper lung, small nodular disease.
- Granulomatous lung diseases: TB, atypical TB, fungal diseases, sarcoidosis, eosinophilic granuloma
- Metastases: eg. thyroid, mucinous adenocarcinomas, melanoma, breast cancer
- Smaller airways disease: eg. bronchiectasis
|
