MAI Infection (Mycobacterium Avium Intracellulare)
Pathophysiology: Generally the commonest atypical tuberculous infection seen. The histologic findings are almost identical to tuberculosis hominis, but generally much less severe, more chronic and indolent. This is a caseating granulomatous lung, airways and pleural infection leading to fibrosis and architectural damage.
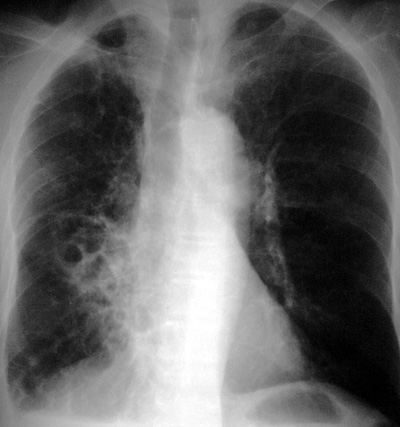
CXR Findings:
Typical CXR patterns:
- nodular lesions in the mid and upper lungs associated with chronic bronchiectasis
- regional bronchiectasis often in the middle lobe or lingula, often with atelectasis, with or without lung nodules in older women (Lady Windemere syndrome)
- superinfection of pre-existing lung cavities or bullae, (eg. due to old tuberculosis hominis)
Often the findings on the CXR are indistinguishable from regular tuberculosis except that the changes are often chronic and indolent with lesser clinical symptoms than seen in tuberculosis.
Clues: The diagnosis is by pathogen identification and clinical/radiologic correlation.
Unlike typical tuberculosis, MAI is often very difficult to treat and eradicate from the patient.
MAI and all atypical tuberculosis ARE NOT community acquired infections. They cannot be spread by person to person or droplet contamination
"Aunt Sophies":
- tuberculosis hominis
- fungal infections
- bronchiectasis of any etiology
|