|

|
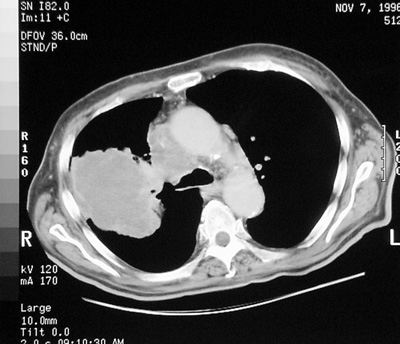
Mediastinal Adenopathy
Pathology: Many diverse diseases can be associated with mediastinal adenopathy and generally the etiology is indeterminate from the plain film images.
Imaging Clues: The patern of adenopathy and associated imaging findings may lead to triaging of the differential diagnosis.
Adenopathy or Not Adenopathy? This is the question.
How to tell hilar adenopathy from prominent enlarged pulmonary arteries:
- Enlarged nodes tend to be lobular, and give the hila a "potato like" contour.
- Hilar adenopathy may be very symmetric and associated with other mediastinal nodes (eg. paratracheal)
- Enlarged pulmonary arteries have the same form as the normal vessels, just dilated.
- Hilum convergence sign: if a vessel can be traced directly into or from a hilar “mass” the mass is vascular
- Hilar overlay sign: If a vessel can be traced through a hilar mass, the mass is not vascular.
Differential Diagnosis of Mediastinal Adenopathy ("Aunt Sophies"):
This is large and should be approached via pathologic categories of disease and be in order of commonality.
- Tumor: primary, metastatic, or lymphoma
- Infection: usually granulomatous (eg. tuberculosis and fungal)
- Idiopathic: sarcoidosis
- Occupational / Inhalational diseases: silicosis, berylliosis
- Benign giant lymph node hyperplasias, Castleman’s disease
- Drugs: dilantin, methotrexate, cyclosporin
- Infiltrative diseases: primary or secondary pulmonary amyloidosis
|
