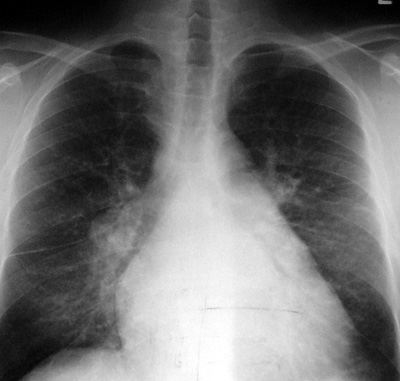
Pulmonary Edema - Interstitial
Pathophysiology: Due to alveolar capillary leakage of
electrolytes and water and in some cases, of larger molecules
into the inter-alveolar walls, interlobular septae, and into the
peri-bronchial and peri-vascular sheaths. The commonest cause
is heart failure. Other causes include hypervolemia,
hypoproteinemic states, acute or chronic renal failure, and any
of the multiple causes of Adult Respiratory Distress Syndrome (ARDS)
Clinical Clues:
1.
The CXR is more sensitive than the best clinician in
detecting interstitial edema.
2.
Clear cut interstitial edema is often not seen in ARDS.
There is fibrinogen and fibrin trapping the free flow of water
and the florid airspace edema masks the interstitial findings.
CXR Findings:
1.
thickened visible interlobular septae (Kerley B
and Kerley A lines)
−
Kerley B lines: parallel lines running along the
outer chest wall, like steps in a ladder
−
Kerley A lines: curvilinear lines starting close
to the hila and extending peripherally
2.
Central peribronchial cuffing
3.
Central perivascular fuzziness
4.
Often enlarged heart, evidence of cardiac or renal
disease (ie. effusions, renal osteodystrophy)
“Aunt Sophies”: The cardinal sign of interstitial edema is
Kerley B lines. Any process which thickens interlobular septae
will produce Kerley B lines.
1.
Fibrosis: many chronic interstitial lung diseases (eg.
UIP)
2.
Chronic bouts of edema leading to fibrosis
3.
Tumor: lymphangitic carcinomatosis
4.
Infection: interstitial pneumonias
5.
COLD (chronic obstructive lung disease), with infection,
fibrosis and septal fibrosis
6.
Rarely, infiltrative processes (eg. amyloidosis)
|