Pulmonary Embolism
The
combination of being potentially lethal coupled with a very
variable or no definite clinical presentation makes this disease
the clinician’s worse fear.
Pathophysiology: A variety of mechanisms leading to
increased coagulability. Often seen in association with bed
rest (post-surgical patient), immobility, venous stasis and leg
edema, and in patients with hypercoagulable states (birth
control medication, cancer patient, protein C/S deficiency etc…)
Clinical Clues: The patient may be symptomatic (shortness of
breath, dyspnea, pleuritic chest pain) or almost asymptomatic
presenting with unexplained lab or CXR findings.
The
clinical index of suspicion plays a pivotal role in the
radiologic workup of the patient.
CXR Findings:
1.
Normal, in nearly 50% patients with proven PE
2.
Prominent central pulmonary artery: Fleishner’s sign
3.
Distal pulmonary artery cut-off and oligemia:
Westermark’s sign
4.
Hampton’s hump: peripheral wedge shaped area of
consolidation
5.
Pleural effusion
6.
Pulmonary edema and failure
Imaging for PE:
1.
CXR: not definitive
2.
Ventilation-perfusion scanning. Usually not very
helpful. May be useful in patients with low clinical suspicion,
normal CXR alongside normal V/Q scan.
3.
**CT thorax with PE protocol (new gold standard)
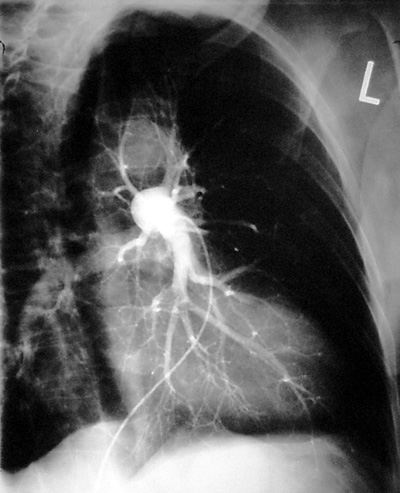
4.
Pulmonary angiography. (old gold standard)
5.
Doppler ultrasound of leg veins
What if we miss a small peripheral emboli?
Controversial: most clinicians state that it is the big emboli
that kill patients. The clinical sequelae of missing small or
subsegmental emboli may not be serious. This issue has not been
resolved yet.
|