Tension Pneumothorax
Pathophysiology: a potentially lethal complication of
simple pneumothorax (PTX). A flap-like valve mechanism develops
involving the parietal pleura such that more air enters the
pleural space on inspiration than exits on expiration. The
result is an increasing inflation of the pleural space with
compressive effects on the lung, large veins, and the heart
(atria). The mediastinum is shifted, there is impairment of
venous return with decrease in cardiac output. Shock and death
may occur if not treated.
Clinical Clues: This is a medical emergency needing
treatment so rule out tension pneumothorax in every suspected
case of pneumothorax
With clinical suspicion, get CXR. Donĺt really need
inspiration and expiration views to make diagnosis; inspiration
views are sufficient.
In
rare situations when CXR is not available and patientĺs
condition warrants, do needle decompression based on clinical
grounds.
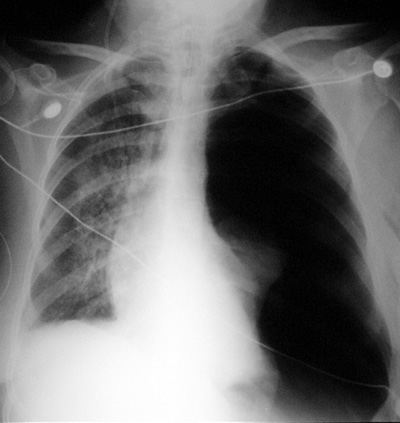
CXR Findings:
-
Visceral pleural
sign with air in pleural space
-
Contralateral
mediastinal shift
-
Tracheal or
esophageal shift
-
In supine patient,
may see superior sulcus sign and mediastinal shift
-
May see evidence of
thoracic trauma: rib fracture, pneumatocele, hemothorax etců
ôAunt Sophiesö: pneumothorax + mediastinal shift = diagnosis
1.
any cause of mediastinal shift without pneumothorax (eg.
volume loss, large effusions)
|