|


|
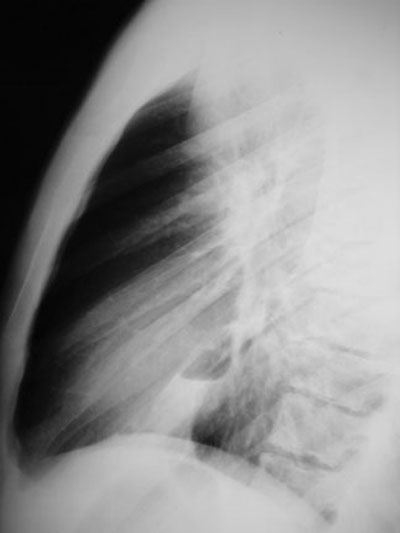
Traumatic Pneumatocele
Pathophysiology: Acute, generally high energy trauma to the
chest wall leading to small airways collapse and regional
“explosion” of the subtended lung. Results in regional areas of
contusion, bleeding and cavitation with the injured lung
communicating with the damaged small airways.
Clinical Clues: Look for more serious associated thoracic
trauma (e.g. aortic injuries, esophageal laceration, tracheal or
bronchial trauma, flail chest, tension pneumothorax, large
hemothorax etc…) which need immediate diagnosis and treatment.
CXR Findings:
-
regional area of
airspace disease with cavitation, may be multiple
-
associated thoracic
trauma (e.g. rib fractures, pneumothorax, hemothorax etc…)
“Aunt Sophies”: gamut of cavitary lung disease
-
infections:
granulomatous and CAP
-
tumour: primary and
metastatic disease (squamous cell)
-
vasculitis (e.g.
Wegener’s granulomatosis)
-
complicated bullous
disease
-
infected
bronchogenic cyst
|
